
If the responsibility is placed on a single person/role—whether a product manager, registration engineer, or clinical specialist—such a person usually cannot cover compliance, product, and clinical evidence simultaneously. The result is multiple rounds of rework, substantial revisions, longer project timelines, unstable report quality, and even a higher risk of clinical deficiency letters.
What does the reality look like? (Based on what I have seen at Siemens Healthineers and Chinese companies)
🔹 Shenzhen MRI Business Unit:the product manager drafts the Clinical Evaluation Report,and the medical officer reviews and approves it. The advantage is close alignment with the product, butliterature/clinical evidence searching and appraisal are challenging, and the writing burden is high.
🔹 Other business units:the clinical team drafts it,and the product manager reviews it. The clinical team is a shared resource,and may not understand the specific configuration/intended use in sufficient depth, so the content can become too generic.
🔹 Locally registered products:the registration team writes the report,with reference to the imported product's CER, which is efficient butcan easily become disconnected from the realities of localization。
After discussions withChinese medical-device companies, I also found that:
▪️ Large companies will havededicated clinical evaluation specialistsresponsible for report writing and evidence management;
▪️ Many small and mid-sized companies still rely onregistration engineersto also prepare clinical evaluation reports.
Even for the same “medical-device Clinical Evaluation Report,” the quality can vary dramatically depending on the division-of-responsibility model—and behind that lies the company'spositioning of clinical evaluation, resource allocation, and risk awarenessthe differences.
So what do the regulations say? (NMPA / MDR / FDA)
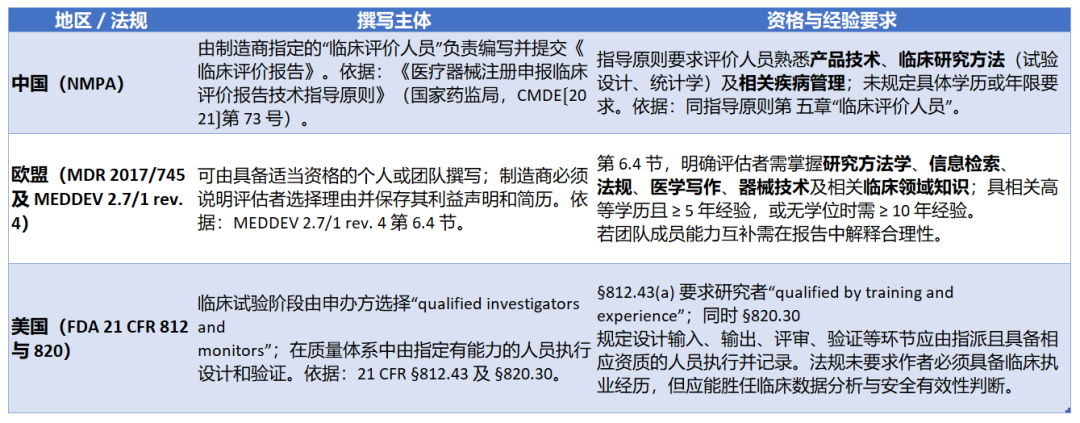 In addition to FDA, both China and the EU set qualification expectations for the person drafting the clinical evaluation. Although they do not specify exactly who must take on the role, it is clear that this role requires expertise in product technology, clinical research, and regulatory affairs. In practice, it is often difficult for companies to find one person with all of these capabilities, which is why the responsibility is often assigned to a single function, such as the product manager or registration engineer.
In addition to FDA, both China and the EU set qualification expectations for the person drafting the clinical evaluation. Although they do not specify exactly who must take on the role, it is clear that this role requires expertise in product technology, clinical research, and regulatory affairs. In practice, it is often difficult for companies to find one person with all of these capabilities, which is why the responsibility is often assigned to a single function, such as the product manager or registration engineer.
Key takeaway, once again: the regulatory intent is not to designate "who should write it," but to requireit to be written correctly, realistically, and completely. The most practical organizational solution is to establisha collaboration mechanism among the Compliance Lead × Product Expert × Clinical/Medical Writer × Biostatistics/Evidence Supportforcollaborative coordination,rather than having a single rolecarry the whole burden”. In the next section, I’ll provide a practicalclinical evaluation co-creation work modelthat reduces rework and improves pass rates,and be sure to plan milestones and deadlines early, the earlier the better,because very often the time runs out halfway through drafting. This is a large document with a huge amount of information,requiring many rounds of review by many sets of eyes to ensure consistency across the information and deliver high-quality output. It is strongly recommended to involve staff with a medical background to provide professional, objective, evidence-based oversight of key information such as the device’s clinical background, clinical claims, and clinical endpoints.
What is my recommendation?
Companies should list all relevant experts involved with the product (R&D, manufacturing, marketing, clinical, etc.) and have them contribute their professional input on schedule when developing the CER (Note: this contribution is not just about handing materials to the report writer; it should involve multiple rounds of discussion on the writing approach, jointly defining the structure and logic, and dividing responsibilities). This matrix-style collaboration ensures that the CER captures knowledge across the device lifecycle, rather than reflecting only one person’s limited perspective. For example, when clinical staff draft the CER, they may lack the ability to assess technical equivalence with comparator products, whereas product engineers can provide that critical technical input, thereby improving the report’s first-pass approval rate.
In practice, large medical device companies typicallyClarify each department's responsibilities in CER preparation, enabling shared accountability:
R&D/Engineering: provide product technical documentation, prepare the technical comparison and impact analysis of differences for equivalent devices, and ensure the technical content of the report is accurate and complete.
Medical/Clinical Affairs: conduct systematic literature searches and appraisal, compile clinical evidence on product safety and effectiveness, and draft the clinical data analysis section.
Registration/Regulatory Affairs: oversee the CER structure and compliance, interpret and implement the latest regulatory requirements, ensure the CER meets regulatory format and key expectations, and provide regulatory strategy recommendations.
Quality/Marketing/Post-market: provide post-market adverse event and complaint monitoring data, collect user feedback and risk information, and support benefit-risk assessment and evaluation of comparable products on the market. The marketing team can also help gather competitor information and position the product's clinical value. Through this division of responsibilities, each function contributes its strengths to the CER, fulfills its role, and shares responsibility for report quality. This collaborative model not only reduces repeated revisions caused by functional blind spots, but also increases cross-functional alignment with the CER conclusions.
CRO collaboration experience and best practices
Leading CROs such as IQVIA, NAMSA, ICON, and PPD have accumulated extensive experience in supporting medical device CER writing and can provide useful lessons for internal collaboration.Working with a CROessentially means bringing in an external "pool of experts" to participate in CER activities, with the advantages of professionalism, efficiency, and no training burden:
An experienced writing team: CROs typically have dedicated medical writing teams that are highly experienced with CER regulatory requirements and literature search and analysis. For example, IQVIA recommends that manufacturers shouldengage experienced CER writers and reviewersin document preparation. These experts can often meet regulatory expectations the first time, reducing the risk of the CER being returned by the Notified Body for rewriting.
Cross-functional support: Large CRO teams include not only medical writers, but also former regulatory reviewers, clinical study design specialists, statisticians, and other roles working collaboratively. Public information from NAMSA indicates that its team includes multiple consultants who previously worked at EU Notified Bodies and are directly involved in CER strategy development and quality review. This multidisciplinary combination helps ensure that the CER meets the latest requirements in both content and format, improving the likelihood of first-pass acceptance.
Mature processes and templates: Through preparing CERs for many clients, CROs have established efficient, standardized processes and template libraries. Working with them allows manufacturers to directly leverage these best practices. For example, consulting firms such as Celegence useLean authoringan approach that optimizes templates, quality control workflows, and team collaboration, significantly shortening document preparation timelines. By engaging a CRO, companies can immediately gain access to theseprocess tools。
flexible staffing: Choosing a CRO means accessing resources on demand without bearing long-term staffing costs. During periods of intensive CER activity, the scope of outsourced work can be expanded, while in routine periods there is no need to maintain additional headcount. In the Vita case study, the FSP model supported more than 600 CERs per year, reduced costs by approximately 30% compared with the traditional outsourcing model, and enabled 85% of team members to work remotely, providing globally scalable flexibility. This shows that making effective use of external partnerships can address CER staffing shortages without increasing internal headcount.
Of course, when companies adopt the CRO model, they should also focus on internalizingexternal expertise, especially during periods when clinical evaluation regulations and standards are being dynamically updated (ISO8969, EU2025/2086): During the process of co-developing CERs with a CRO, internal staff should be involved in learning so they can gradually master advanced collaboration methods, templates, and tools. In the long term, building an in-house team of CER specialists and creating a dual-driver model of “external expertise” + “internal expertise” will better strengthen the organization’s overall capabilities.
At the end of this article, I will also attach the Notified BodyBSI White Paper on Clinical Evaluation Practicefor your reference, to help guide efficient demonstration of the safety and clinical performance of medical devices in Clinical Evaluation Reports. Comments and discussion are welcome.
#Clinical Evaluation #Regulations/Standards